






Strabismus or strabismus is a disease in which both eyes do not look in the same direction at the same time, in other words, deviation of the visual axis of the eye to the side.
Origin and division of the disease:
There are two basic forms of strabismus:
1. Concomitant strabismus (lat. Strabismus concomitans) is one in which the eye whose visual axis is shifted in any direction follows the movements of the other eye. Let’s take for example a person who looks straight ahead with the healthy right eye while looking towards the nose with the other eye, the left. If that person directs the gaze of the healthy eye to the left and the left eye simultaneously moves outward but remains in the same relationship to the right eye (thus looking relatively more towards the nose), we speak of concomitant strabismus. Here, the diseased eye therefore follows the healthy one, but always maintains an equal relationship (deviation) to it.

Concomitant strabismus, forward gaze.

Concomitant strabismus, looking to the left.
2. Paralytic strabismus (lat. Strabismus paralyticus) , incomitant strabismus is one in which there is a weakness of a certain muscle that moves one eye, so when looking straight ahead there is a deviation of the visual axis in relation to the healthy eye. The size and direction of such a deviation depends on which muscle is affected. If the healthy eye moves to the side, the movement of the diseased eye can be symmetrical and complete or only partial, or even none at all. It depends on the direction of action of the affected muscle. As the anatomy and function of the muscles that move the eyeball is very complicated, I will not go into details here, but it should only be remembered that in paralytic strabismus, the diseased eye does not always follow the healthy eye. The squint angle therefore changes.
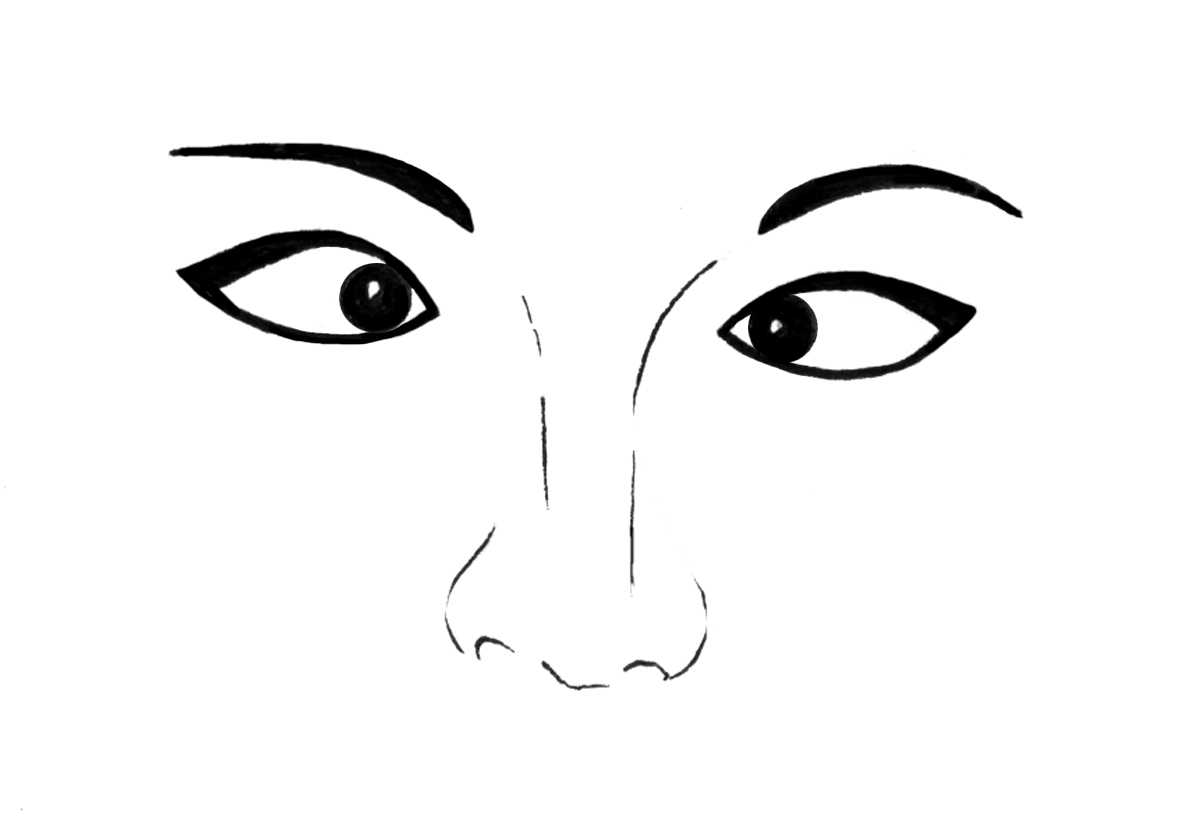
Paralytic strabismus, forward gaze. The right eye has limited movement.

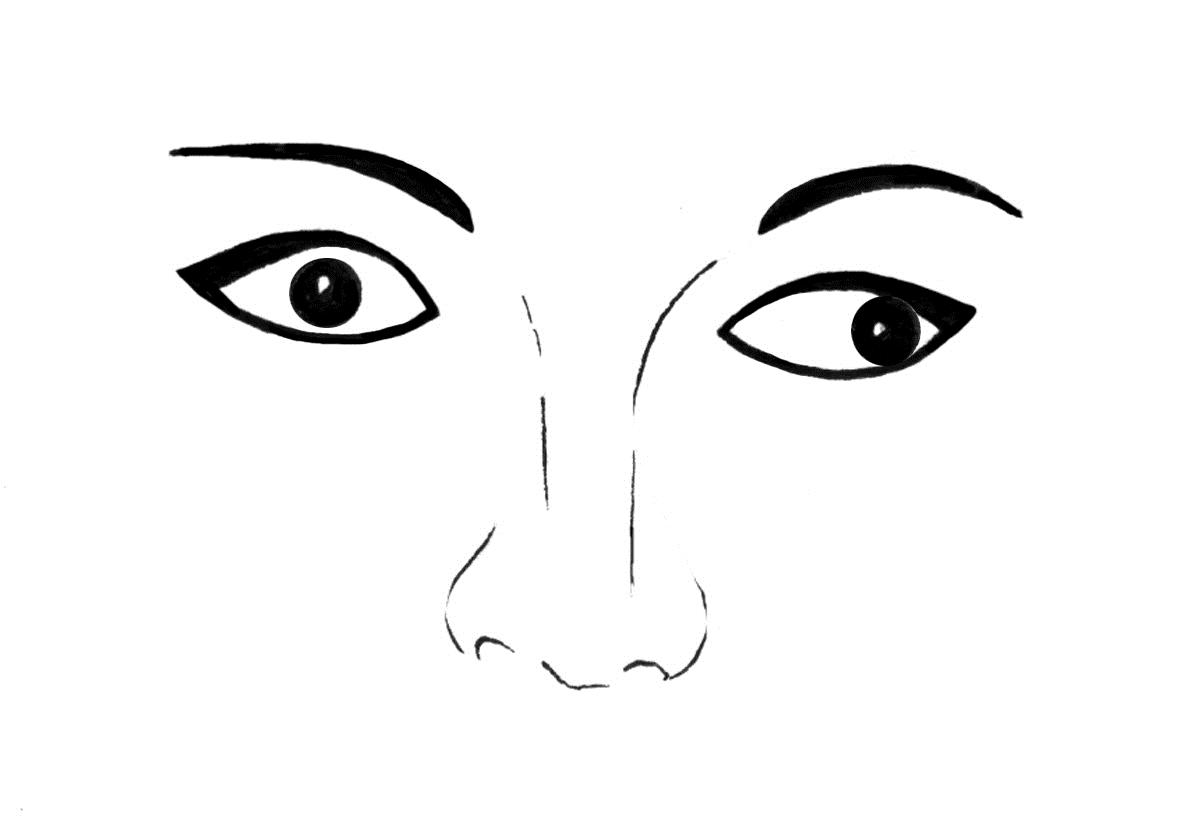
Paralytic strabismus, looking to the right. It is visible that only the left eye has moved while the right one is still in the same position.
Concomitant strabismus
This type of strabismus occurs almost exclusively in children, mostly up to two years of age. The disease is not common and affects about 5% of children. Its causes are manifold, and their basis lies in the fact that, at an early age, vision and coordination of eye movements are not developed, so disorders easily occur. Genetic factors play a big role in this, i.e. heredity, poor vision in one or both eyes, either due to not wearing glasses when they are needed, or due to other diseases that weaken them, and a large difference in diopters between the right and left eye (anisometropia). Due to this difference in diopters, a difference in the size of the image obtained on the retina can occur (aniseikonia).
The place of clearest vision is the macula. In picture X, we see that the image of the object that we look at with the healthy eye falls exactly on the macula, while at the same time the image of that object is in another place on the retina of the diseased eye. In the long run, this can have serious consequences. Namely, due to double images (we have the appearance of two objects instead of one) and the confusion that arises in the brain that “analyzes the results”, the brain can subconsciously turn off one eye, which is why vision simply does not develop in it and it remains visually impaired forever (amblyopic, lat. Amblyopia). Another, slightly better possibility is that the area of the retina where the image falls takes over the role of the macula, which eliminates the double images, but that area will never have the sensitivity or vision quality of the macula.
We distinguish two types of concomitant strabismus:
 Convergent strabismus (lat. Strabismus convergens) in which the diseased eye is directed inward, i.e. toward the nose. It occurs most often at the age of up to 7 years, and it can be congenital, i.e. visible already at birth, or acquired, so it becomes visible after a few years of life.
Convergent strabismus (lat. Strabismus convergens) in which the diseased eye is directed inward, i.e. toward the nose. It occurs most often at the age of up to 7 years, and it can be congenital, i.e. visible already at birth, or acquired, so it becomes visible after a few years of life.
 Divergent strabismus, (lat. Strabismus divergens) in which the diseased eye is directed outwards. It occurs most often in adults as a result of a stronger weakening of vision in one eye.
Divergent strabismus, (lat. Strabismus divergens) in which the diseased eye is directed outwards. It occurs most often in adults as a result of a stronger weakening of vision in one eye.
Paralytic strabismus
Paralytic strabismus, i.e. the one in which eye movements are weakened, can be present at birth or develop later in life. Congenital strabismus is caused by possible inflammation of the brain while still in the womb, other brain disorders or trauma during the passage of the child through the birth canal. At a later age, potential factors that lead to this disease are diabetes, trauma, strokes, brain tumors, arteriosclerosis, etc.
Paralytic strabismus can be divided into three basic groups:
- Neurogenic, i.e. those whose cause is a disorder of muscle innervation (innervation, to put it simply, is “supplying” the muscle with nerve impulses, i.e. giving “instructions” for its movement). It is therefore clear that each muscle is driven by a corresponding nerve. The eye muscles, the six movers of the eyeball, are innervated by three cranial nerves. If they are injured or in some other way functionally changed, either in their origin in the brain, or in their course, they lose control over the muscle and the ability to manage it. In such a situation, the muscle is completely limp and without function, so it cannot move the eye.
- Myogenic are all those caused by muscle disease. These include muscle inflammation, changes in dysthyroid orbitopathy, i.e. thyroid hormone disorders, myasthenia gravis with involvement of the eye muscles (in this disease there is an inability to transmit signals from the nerve to the muscle) and some other conditions.
- Mechanical factors make up a broad group in which orbital bone fractures, where a broken piece of bone gets stuck into the muscle, making it impossible to move, and large bleeding and swelling that have a similar effect, should be emphasized.
Symptoms of strabismus:
Based on what was said earlier, we can conclude that the symptoms depend on the type of strabismus and the direction of movement. In concomitant, non-paralytic strabismus, the most common symptom (and often the cause!) is impaired vision in one eye. The appearance of double images, which are also relatively common in strabismus, depends on whether the macula has retained its function, i.e. whether the brain interprets the rays of light from the viewed object falling on it as “straight ahead” or whether another area of the retina has taken over the role of the macula. If it is, there will be no double image because that area now receives the same light impulse as the macula of the other side, and the brain analyzes it in the same way. If, on the other hand, the macula retains its central role, then due to its new position, it receives a different light impulse than the macula of a healthy eye, resulting in unbearable double images (see picture). In order to protect the organism from double vision, the brain simply “turns off” one eye and the person sees with only one eye. Such long-term disconnection of one eye leads to the fact that the vision in it simply does not develop, so such a person remains visually impaired forever. This is explained by the fact that a child’s vision develops until the age of eight or at most ten, so all disorders that occur during that period can result in underdevelopment of vision (amblyopia).
In paralytic strabismus, a special position of the head is also emphasized, with which the patient tries to reduce the role of the affected muscle that moves the eye and thus reduce double images.
Establishing a diagnosis:
It is not necessary to emphasize the fact that strabismus is very easy to notice by careful observation. Establishing a basic diagnosis of strabismus is therefore very quick and easy. On the other hand, determining the type of strabismus as well as all the potential factors that led to it requires a lot of research. It is essential to do a complete examination of the eye, i.e. all its structures with a special emphasis on the cornea, lens, vitreous, retina and optic nerve, i.e. those structures which, if they are changed, most directly affect the weakening of visual acuity. Visual acuity in children needs to be determined with the help of fluoroscopy. This is a method in which the pupil is first greatly expanded and completely excludes the influence of the ciliary muscle on the lens. Then, in complete darkness, with the help of a small light source and a mirror, the diopter is determined. In order to determine the mobility of the eye muscles, the examinee should direct his gaze in 9 directions while fixing a pencil or other similar object. The directions are straight, up, down, left, right, up left, up right, down left and down right. The appearance of double images, i.e. noticing two pencils in certain positions, will provide valuable information for a more detailed determination of the type of strabismus. With the help of the cover-test, the existence of even the smallest outages can be determined with great precision, and its advantage lies in the fact that it can be performed even with very young children and people who do not cooperate well. When performing it, the hand alternately covers one eye and the other while the examinee looks at the given object. When the eye is revealed, the shift with which that eye begins to focus on the object is clearly visible while the other is covered. We will only list the remaining tests because they are too complex to describe. These include fixation tests (the area of the retina that focuses the viewed object), tests using the Madox cross and Madox wings, synoptophores, stereo vision tests, prism tests and many others.
Treatment:
The basis of any strabismus treatment is determining the correct diopter in order to achieve the sharpest possible vision. In simplified terms, it can be stated that the first stage of treatment is actually the treatment of low vision, pleoptics. For this purpose, there are a large number of methods and techniques that include covering (occlusion) the better eye, and sometimes the worse eye in certain periods, and performing certain exercises. They try to achieve that the macula is the one that fixes the image (and not some other part of the retina, as is often the case, see the picture), and that vision is improved to the greatest extent possible. In the second phase of treatment, the eyes are tried to be brought into a normal, parallel position, and all the techniques used for this purpose are collectively called orthoptics. Here, too, there are a large number of exercises that achieve and strengthen fusion (fusion is the merging of the image that comes from each eye separately into a single image in the brain). Other methods include occlusions and wearing prismatic glasses.
Surgery is the ultimate but by no means omnipotent method in the treatment of strabismus. It is applied only when it is not possible to achieve healing with other methods. Usually, it is enough to operate on only the strabismic eye, but in certain situations it is necessary to operate on both eyes. After the operation, it is still necessary to carry out certain exercises in order to maintain the new condition. The time for the procedure is not determined by any rule, but is determined on a case-by-case basis. There are several arguments for earlier surgery (around the second year of life), as well as those that speak in favor of later surgery. In order to make a decision, it is necessary to consider the condition of the eye in detail.
What is particularly important to emphasize is that the treatment of strabismus is very difficult and long-term and does not always produce the expected results. Not only the doctor plays a role in it, but also the child and especially his parents. Only with the cooperation of all the aforementioned, a good basis is obtained for the implementation of all the previously mentioned treatment methods.
Literature:
M.Sc. sc. Pavan Dr. Joško, “Eye Diseases”, Zagreb 2003.
